

Case Spotlight: Hardware | Richard Driessnack, MD
67 y/o female with history of a left distal femur fracture in 2009, treated with retrograde locked IM nail. Fracture healed well, but post-traumatic arthritis developed in the left knee. Conservative treatment with injections, physical therapy, and anti-inflammatory medications failed to control her symptoms of pain, stiffness, and functional impairment.
Patient History
Product: iTotal PS
Gender: Female
Age: 67
BMI: 43.6
Deformity: 10˚ of varus on standing long-leg alignment CT scan, 22˚ flexion contracture on long-leg standing CT scan
PSHx: ORIF left distal femur, hysterectomy, benign tumor excison ankle
PMHs: Obesity, Hypertension, Hypercholersterolemia, Type 2 Diabetes, Anemia, Osteopenia

Pre-Op Exam
Symptoms: Pain and stiffness in the left knee, cannot walk >1/2 block, avoids stairs, limits grocery shopping, considers herself greatly impaired functionally
Location of symptoms: Medial joint line tenderness
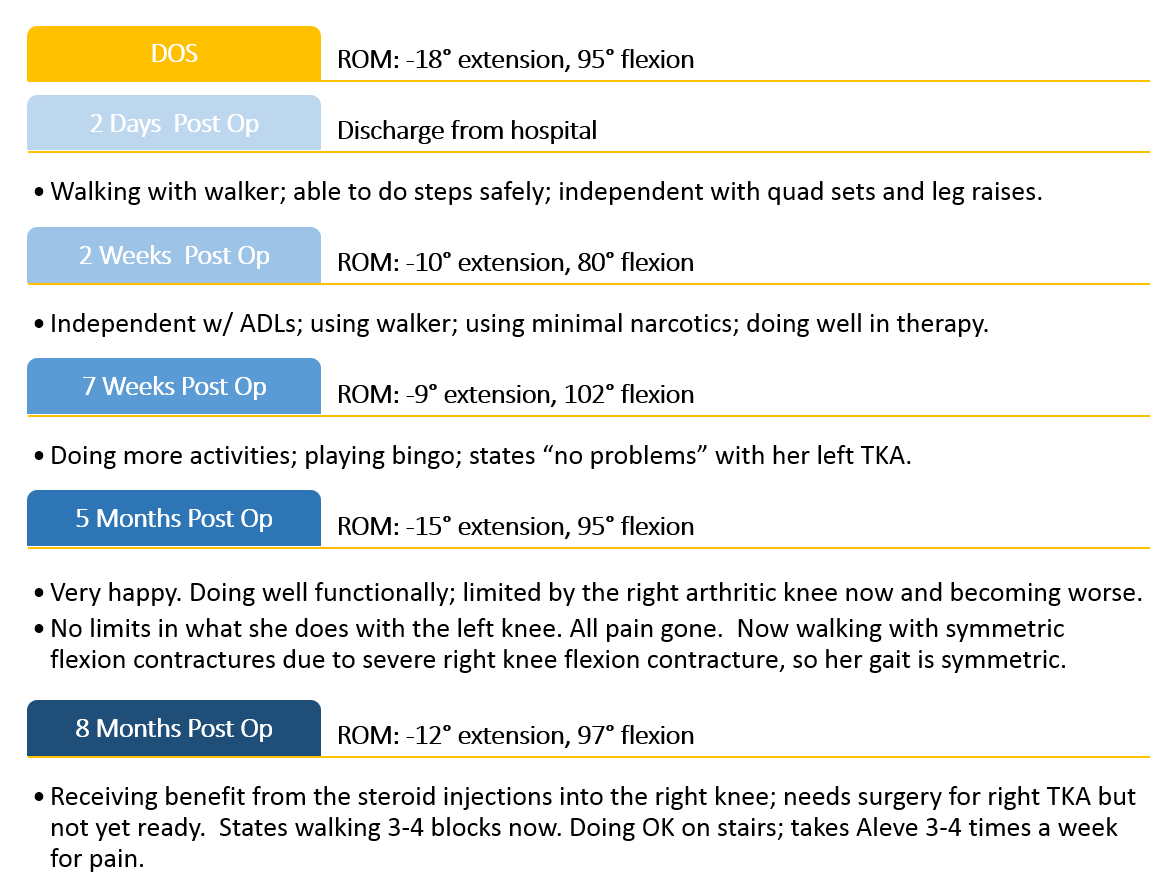
ROM: -18˚ extension, 95˚ flexion
Alignment: 18˚ of varus on standing long-leg alignment CT scan, 22˚ flexion contracture on long-leg standing CT scan
Ligament exam
ACL: stable
PCL: stable
LCL: stable
MCL: stable
Additional concerns: Very obese patient. Significant flexion contracture in both knees.
Motion Right knee is extension -15˚, flexion 98˚. Motion Left knee is extension -18˚, flexion 95˚. Concern will be for flexion contracture correction and maintenance of same in post-op phase, given opposite knee also has flexion contracture
Why Conformis?
The presence of previous hardware in the femur made this patient an excellent patient for consideration of a custom Conformis PS knee. Avoidance of having to remove the IM nail with all locking screws in an obese patient is a huge benefit to the overall morbidity of the case, and hence to give the optimum opportunity for recovery of motion in this case. The PS design allows me to fully expose and debride the posterior capsular area, release tight soft tissue, remove any offending osteophytes, and attain as much extension as possible.
Surgical Objectives
- To avoid nail extraction during the femoral component placement
- To correct flexion contracture
- To improve overall flexion
- To achieve soft tissue balance and a stable knee
iView Pre-op Plan
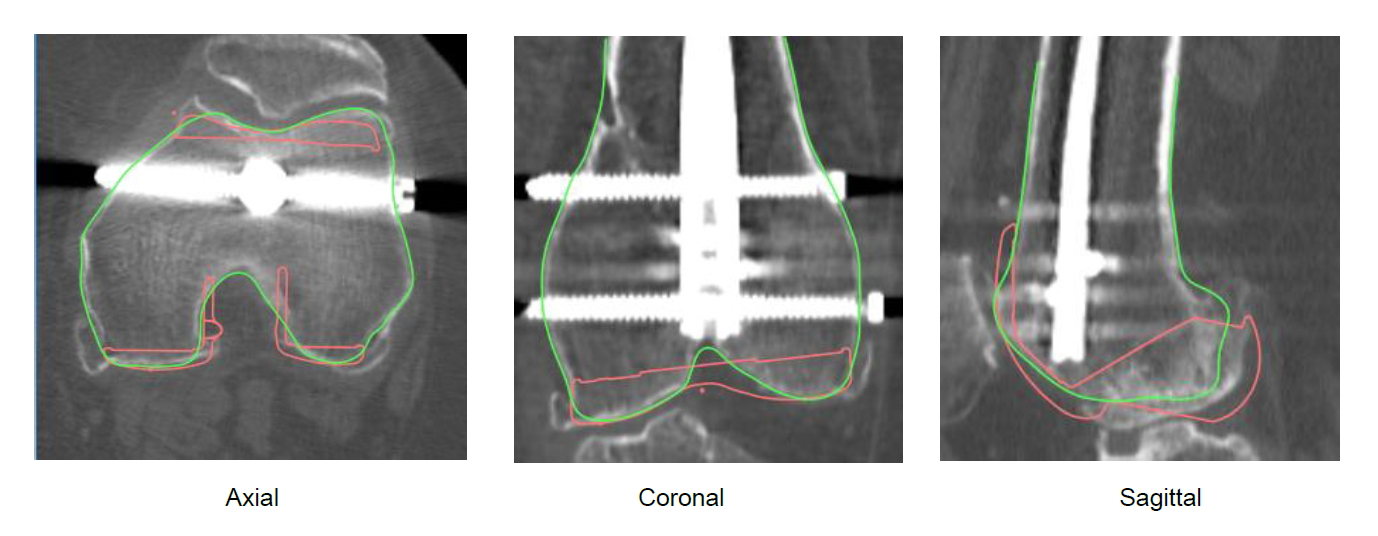
Notable Condition: Hardware Discovered
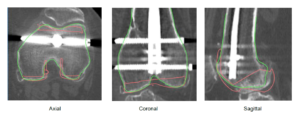
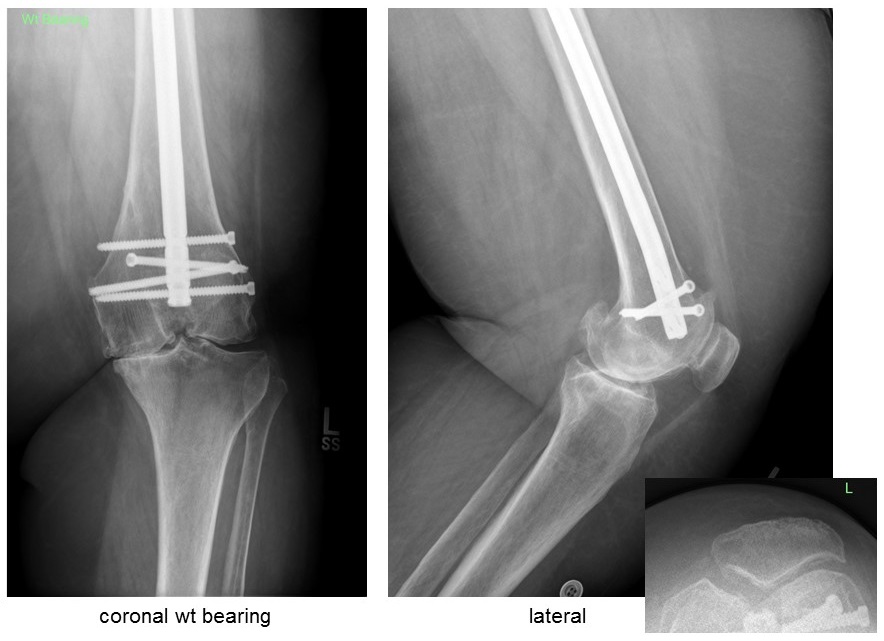
During the process of designing the implants, hardware was discovered. Hardware is not incorporated into the design of the iJigs or implants. It is assumed that interfering hardware will be addressed during surgery.
Dr. Driessnack: “Intra-op noted 2 mm of clearance between the distal end of the IM nail and the femoral component, enough clearance to execute the procedure successfully and avoid increased morbidity of nail removal.”
Intraoperative Details
Surgical Technique: Measured Resection
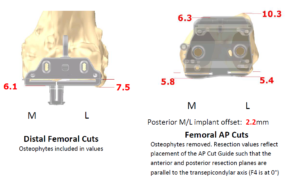
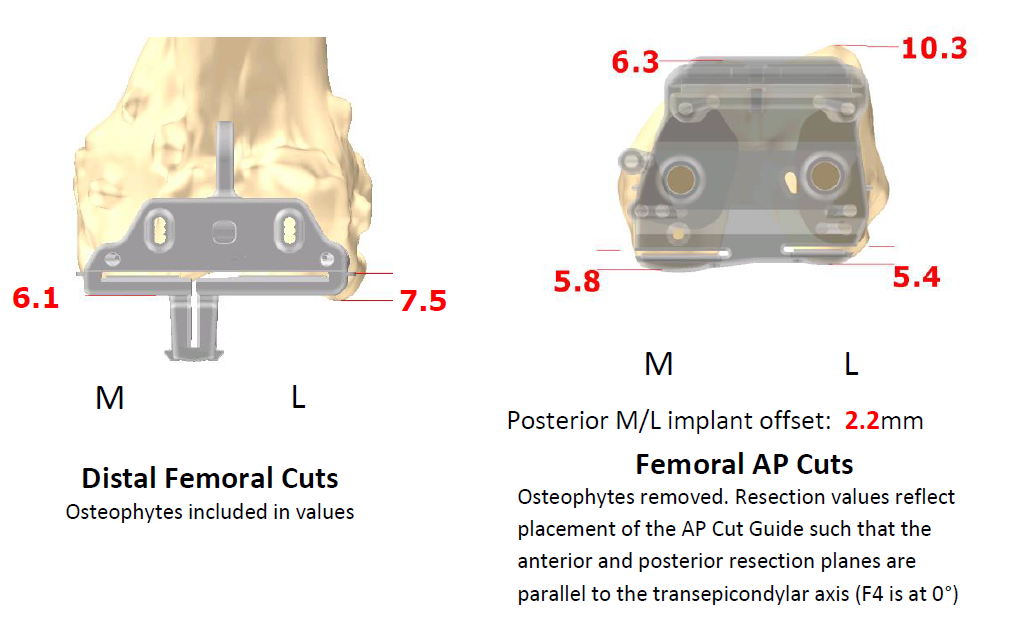
Distal Offset: 0.7mm
Femoral Resection: +2mm
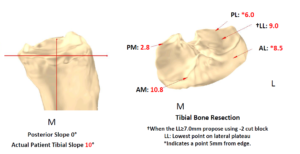
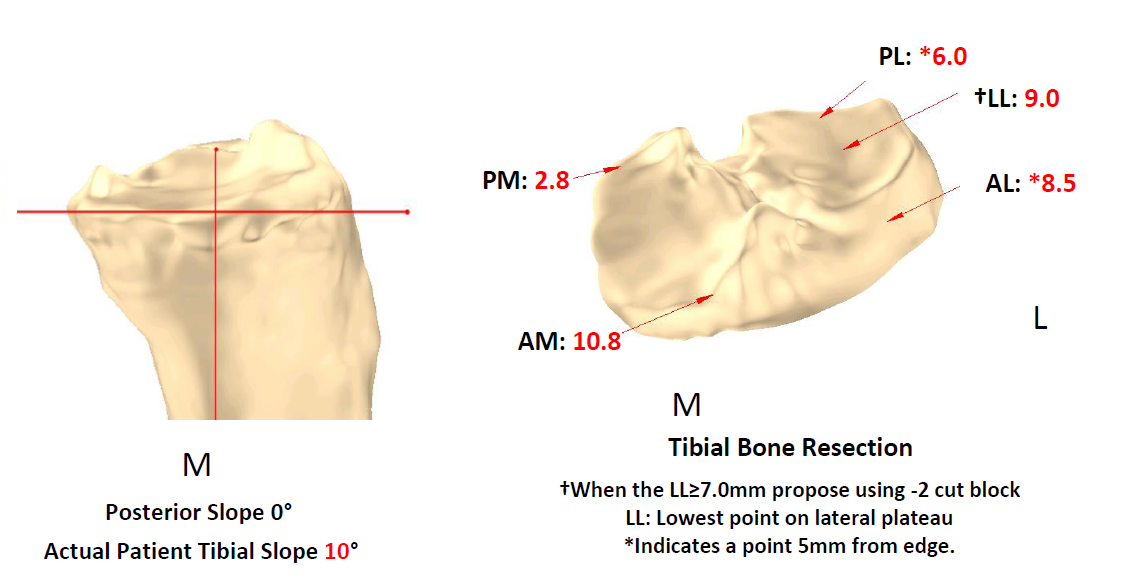
Tibial Resection: At plan
Final Poly: 6mm
Patella: 35mm Conformis patella
Additional Notes
- Spinal anesthesia, adductor canal block, intra-articular bupivacaine and toradol.
- Ligament balancing technique used: Medial release was routine, no lateral patellar release was needed, additional bone resection done to gain full extension.
- Surgical Approach: Standard midline incision, medial parapatellar capsular incision, measured resection.
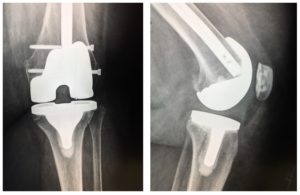
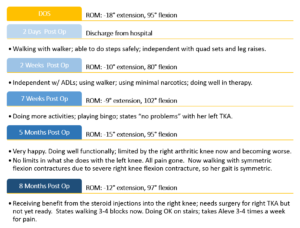
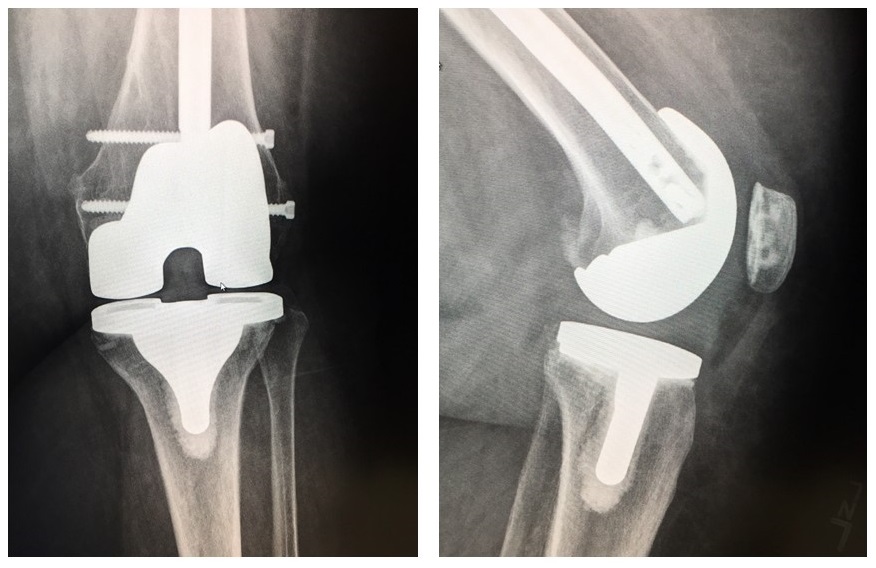
Post-op Results
Surgery Performed by:
Richard Driessnack, MD
OSF Orthopedics
Peoria, IL
Conformis user since 2015

All Case Spotlight Images
About Conformis
We start with a simple idea: make the implant fit the patient rather than force the patient to fit the implant
About Conformis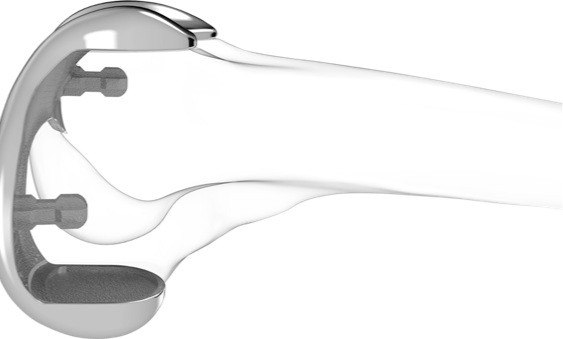
Surgeon Resource Center
Take an in-depth look at product information, clinical data, and the experiences of other surgeons
Surgeon Resource Center