

SHAPE DRIVES STABILITY
 Instability leads to implant failure
Instability leads to implant failure
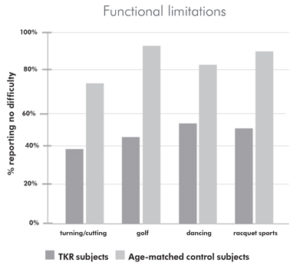
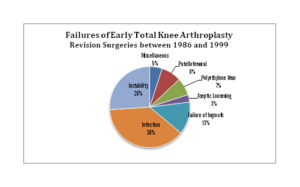
Not only is instability a cause of functional limitations, it is also associated with a 3.7x increase in the risk of implant failure.5 In a series of 279 patients who had revision surgery within 5 years, instability was the 2nd leading cause of early failure.6
The patient-specific solution
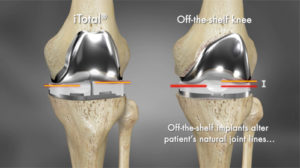
 By respecting the patient’s natural J-curves, corrected for deformity, Conformis replicates the femoral offset in the implant design. Dual-balancing™ offsetpoly inserts allow for broader contact area and the maintenance of those medial and lateral joint lines. The iTotal®, in an in vivo study of patient kinematics, better approximated natural kinematics compared to both modern and legacy off-the-shelf total knee implant designs and exhibited motion patterns more closely resembling a normal knee.7
By respecting the patient’s natural J-curves, corrected for deformity, Conformis replicates the femoral offset in the implant design. Dual-balancing™ offsetpoly inserts allow for broader contact area and the maintenance of those medial and lateral joint lines. The iTotal®, in an in vivo study of patient kinematics, better approximated natural kinematics compared to both modern and legacy off-the-shelf total knee implant designs and exhibited motion patterns more closely resembling a normal knee.7
One potential reason for this difference is that standard knee replacement designs don’t preserve the patient’s condylar geometry, and their medial and lateral joint lines. As a result, off-the-shelf implants, including single radius designs, have been shown to alter kinematics.8
https://conformis.wistia.com/medias/v06qray367?embedType=async&videoFoam=true&videoWidth=640
2: Pagnano, et al; Flexion Instability After Primary Posterior Cruciate Retaining Total Knee Arthroplasty. Clinical Orthopaedics and Related Research; 1998, 356: 39-46
3: Noble, et al; Does Total Knee Replacement Restore Normal Knee Function? Clinical Orthopaedics and Related Research; 2005, 431: 157-165
4: Whiteside, et al; The Influence of Joint Line Position on Knee Stability After Condylar Knee Arthroplasty. Clinical Orthopaedics and Related Research; 1990, 259: 146-156
5: Fang, et al; Coronal Alignment in Post-operative TKA: Just how important is it? Journal of Arthroplasty; 2009, 24 #2: 39-43
6: Fehring, et al; Early Failures in Total Knee Arthroplasty. Clinical Orthopaedics and Related Research; 2001, 392: 315-318
7: Kurtz, et al; In Vivo Kinematics for Customized, Patient Specific Vs. Two Generations of Traditional TKA During Various Activities. Presented at the British Association for Surgery of the Knee 2016 Annual Meeting.
8: Bull, et al; Component Rotation and Anterior Knee Pain after Total Knee Arthroplasty. Clinical Orthopaedics and Related Research; 2008, 466: 2491-2499